In pediatric practice, the transition from acute volume resuscitation to maintenance therapy requires a precise shift in both fluid tonicity and additives.
For pediatric rehydration, selecting the appropriate fluid depends on whether you are providing volume resuscitation (bolus) or maintenance therapy.
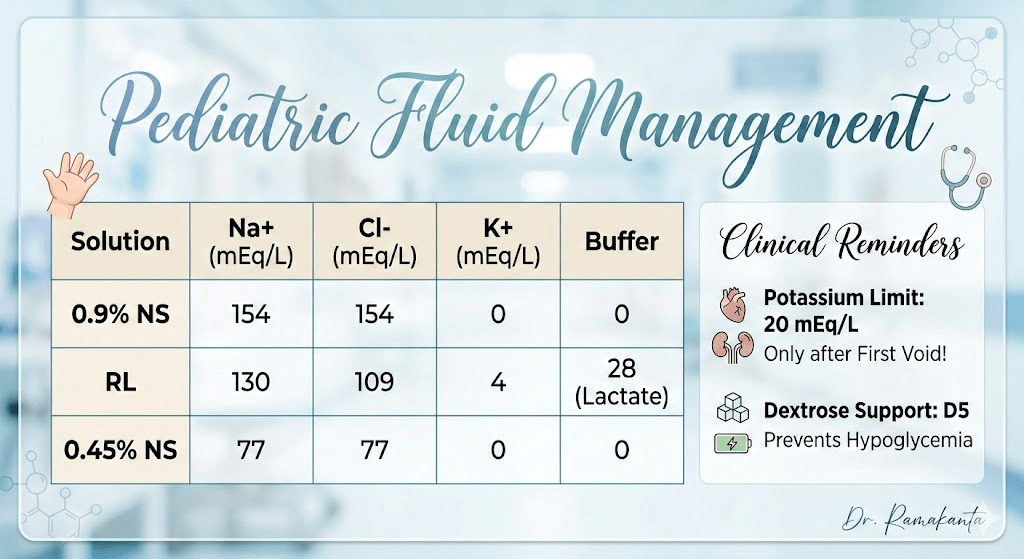
The following table compares common crystalloids. Note that standard “off-the-shelf” fluids like Normal Saline (NS) or Ringer’s Lactate (RL) do not typically contain Dextrose or sufficient Potassium for maintenance, so these must be added or ordered as specific premixed pediatric solutions (e.g., D5 ½ NS + 20 mEq/L KCl).
| Solution | Na+ (mEq/L) | Cl- (mEq/L) | K+ (mEq/L) | Buffer |
|---|---|---|---|---|
| 0.9% NS | 154 | 154 | 0 | 0 |
| RL | 130 | 109 | 4 | 28 (Lactate) |
| 0.45% NS | 77 | 77 | 0 | 0 |
Critical Additives for Pediatrics
In a clinical setting, once initial resuscitation is complete and the patient has demonstrated adequate urine output, the focus shifts to maintenance requirements.
1. Potassium (K+) Supplementation
- Standard Addition: Usually 20 mEq/L of KCl is added to maintenance fluids.
- Indication: To prevent hypokalemia during fasting or prolonged rehydration.
- Safety Check: Never add Potassium until voiding (urine output) is confirmed to avoid life-threatening hyperkalemia, especially in dehydrated children.
2. Dextrose (Energy Support)
- Standard Addition: 5% Dextrose (D5) is typically added to maintenance fluids for children.
- Purpose: To prevent hypoglycemia and inhibit ketosis (lipolysis) while the child is NPO (nothing by mouth).
- Note: D5 adds approximately 170 kcal/L, which provides about 20% of a child’s normal caloric needs—enough to spare protein breakdown but not for long-term nutrition.
Clinical Summary for Rehydration
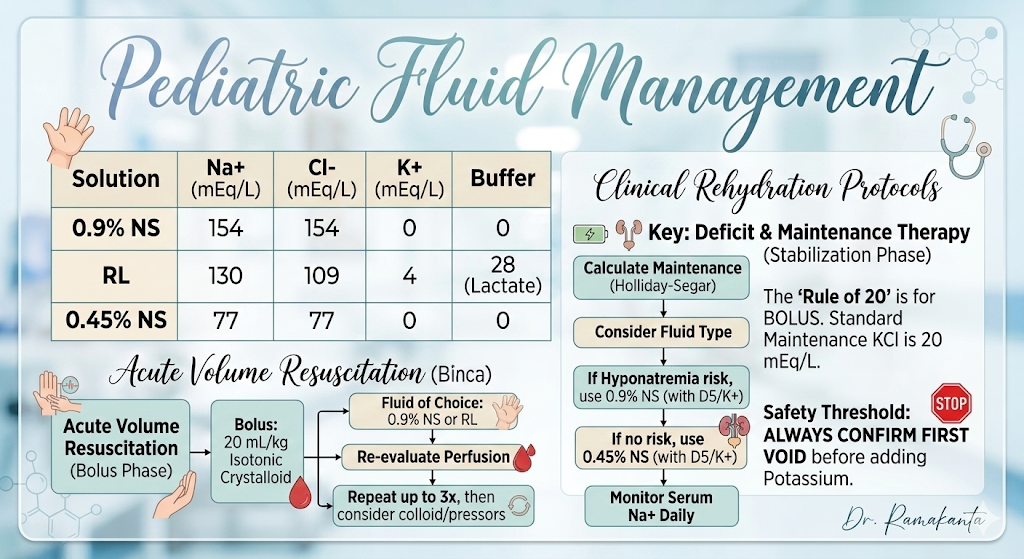
- Phase 1 (Emergency): Use Isotonic fluids (NS or RL) for boluses (20 mL/kg) to restore perfusion. No Dextrose or K^+ is needed here.
- Phase 2 (Maintenance): Transition to D5 ½ NS or D5 NS with 20 mEq/L KCl.
- Note: Recent pediatric guidelines increasingly favor Isotonic Maintenance (using 0.9% NS as the base) to reduce the risk of hospital-acquired hyponatremia.
| Phase | Primary Goal | Recommended Fluid | Key Additives |
| Resuscitation | Restore Perfusion | 0.9% NS or RL | None (Avoid Dextrose/K+) |
| Deficit/Maintenance | Replace losses & Maintain | 0.9% NS or 0.45% NS | D5 (Energy) + 20 mEq/L KCl |
Essential Clinical Reminders
- The “Rule of 20”: 20 mL/kg boluses for resuscitation. In cases of cardiogenic shock or severe malnutrition, this is often reduced to 5–10 mL/kg.
- Potassium Threshold: Always confirm the “First Void” before adding KCl to the bag to ensure renal clearance is functional.
- Glucose Balance: While D5 prevents ketosis, it does not provide full caloric support. For long-term NPO status, transition to TPN is usually considered.
- Isotonic Shift: Current AAP clinical practice guidelines generally favor isotonic fluids (e.g., 0.9\%NS) for maintenance in most hospitalized children to prevent the development of hyponatremia.
Clinical Case Study
The 10 kg Challenge patient: 1-year-old infant, 10 kg.Presentation: Moderate to severe dehydration secondary to acute gastroenteritis. Sunken fontanelle, delayed capillary refill (3 seconds), and decreased skin turgor.
Phase 1:
Emergency Resuscitation : For a 10 kg child in shock or severe dehydration, the “Rule of 20” is your first move.
Action: Immediate IV bolus of 0.9% Normal Saline or Ringer’s Lactate.
Volume: 20 mL/kg \times 10 kg= 200 mL over 20 minutes.
Goal: Restore perfusion. Repeat if necessary until hemodynamic stability is achieved.
Phase 2: Calculating Maintenance (Holliday-Segar)
Once the bolus has stabilized the patient, we calculate the 24-hour maintenance requirements. Rule: 100 mL/kg for the first 10 kg.
Calculation: 100ml times 10 = 1,000 mL over 24 hours.
Hourly Rate: 42 mL
Phase 3: The Transition to Oral (The Goal)
As the child improves and vomiting subsides, we transition to the oral route while the IV remains in situ for safety.IV Additives: Once the child has their “First Void,” add KCl (20 mEq/L and ensure D5 is present to prevent ketosis.
Oral Rehydration (ORS): Begin small, frequent sips of ORS (5 to10 mL every 5 minutes).
Integration: For every loose stool or episode of emesis, supplement with an additional 10 mL/kg (100 mL) of ORS to keep up with ongoing losses.
